
Welcome back
In the beginning of this article we saw how this drug was conceived. By observing the fact that young boys with the genetic mutation for 5a reductase, had reduced prostate size and development. The key here is that DHT is needed for normal development and that enlargement does not occur until later in life.
What do we know about testosterone levels later in life? They start to decline we are told.
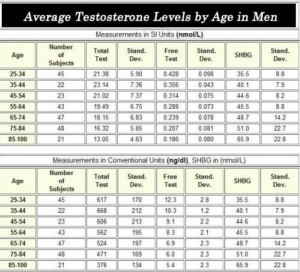
We are looking at total test (testosterone) and free test. Also of interest is SHBG = Sex Hormone Binding Globulin. SHBG binds the sex hormones, thus making the amount of free testosterone which is available less. SHBG appears to increase as men age. The other theory is that SHBG can activate receptors when testosterone (and other hormones, DHT, estrogen etc. – please see the section on phytoestrogens and SHBG for more information on this- Should be out next week) is bound to it, thus it acts to increase the time the testosterone is available in the body. The difference is that the physical outcome is NOT the same as testosterone or DHT alone (without binding to SHBG first).
In the end, if SHBG binds testosterone and DHT, you have more free estrogen available, but again there is a twist – read the phytoestrogens and SHBG section, that should be available next week- to find out more.
Couple this with all the estrogen mimicking compounds out there like, medications, chemicals in plastics, pollution in air, chemicals in drinking water, receipt paper (see further below) etc. and what do we have?
We have what is known today as estrogen dominance. Many people have heard of this, but many more have not. What is surprising is that even out of those that have heard of this, nearly none do anything about it, or know where to start.
That’s OK, we will guide you.

Are you a fast food king?
Here is a list of some of the symptoms of high Estradiol (E2), the dominant estrogen out of the three main ones, the other two being Estrone (E1) and Estriol (E3)
You don’t have to experience all of the symptoms to know that you have high E2:
- * Depression
- * Trouble reaching an orgasm
- * Erectile dysfunction
- * Anxiety
- * Panic Attacks
- * Prostate problems
- * Gynecomastia
- * Water Retention
- * Dizziness/Vertigo
- * Increased Blood Pressure
- * Decreased Libido
- * Asthma like issues (due to increased water retention around the lungs)
- * Trouble sleeping at night – waking up multiple times per night
- * Lack of Libido
- * Crying while watching TV shows/movies
- * Easier to get angry (think PMS)
- * Insulin Resistance (getting tired after eating a meal – if left
untreated, it can lead to Type II Diabetes) - * Larger stomach
- * Redness on the face and/or chest
- * Feeling hotter than everybody else
- * Thinner skin/bleeding easier
What has high estrogen got to do with prostate enlargement? Apparently a lot:
Endocrine Environment of Benign Prostatic Hyperplasia: Prostate Size and Volume are Correlated with Serum Estrogen Concentration
“Estrogen plays an important role in the development of benign prostatic hyperplasia (BPH), as has been shown in both experimental and clinical studies. To determine the endocrine environment of BPH, serum total testosterone (Total-T), free testosterone (Free-T), and estradiol (E2) concentrations were measured, and the relationship between these levels and prostate size and volume was analyzed. Blood samples were collected from subjects who attended the mass screening for prostate disease performed by our institute.
No significant correlations were found between Total-T levels, Free-T levels, and prostate size, as determined by digital rectal examination.
However, E2 levels and the ratios for E2/Total-T and E2/Free-T were significantly correlated with prostate size. To confirm these relationships, prostate volume was calculated from trans-rectal ultra-sonographic images. E2 levels and these two ratios were, indeed, highly correlated with prostate volume. These results suggest that an estrogen-dominant environment plays an important role in the development of BPH.”
In other words, men with highest levels of testosterone and lower estrogens had the least prostate enlargement. And estrogen dominance was the cause of prostate enlargement. By the way, women don’t have prostates but they do have breasts, ovaries and uteruses. The rise of cancers involving these female tissues is also sky rocketing, most probably for the same reason the prostate is enlarging in males and turning malignant.
What about DHT (dihydrotestosterone)?
Did we not just read before that the whole point of the drugs Finasteride, Proscar, Propecia etc. was to reduce prostate size by blocking conversion of testosterone to DHT, and that the drug does this by competing for and specifically inhibiting the enzyme 5a-reductase II?
Well yes, that is what the drug does, they tell us, and it was initially (and currently) marketed for prostate enlargement, as well as androgenetic alopecia after they observed the effect it had on bald heads.
But again, here is some research that shows DHT does not cause prostate enlargement.
In fact DHT, reduced prostate size by 15% over about 2 years in this study! The second block of text says it all.
Transdermal Dihydrotestosterone Treatment of ‘Andropause’
As a side note, “andropause” occurs in a sick population. Some drop off in androgens might be normal with ageing, but not to the level where men have higher estrogens than women! See the ratio of DHT to testosterone in the graph on the following pages.
The diseases present in the male population today, mainly cancer + prostate enlargement + cardiovascular + diabetes + metabolic syndrome were not there in the past at the level present today. (We know diabetes was present, at least the type II, adult onset, (insulin resistance) as the Greeks, from where we got the name “diabetes” = one who travels through (the crowd), noticed that some in the agora (market place) would hurry off due to polyuria= frequent urination, and so they called them “diabites”= one who hurries/walks off through the crowd= enters through something (sea or forest etc.). We also know that baldness was present in the ancient world, but I doubt it was at the level we see today, just like the diseases mentioned.
Obviously something has caused this rise in the diseased state, and it is not your genetics! If it was due to genetics alone, this disease trend would wipe out the entire human race in the next few hundred years. The answer lies elsewhere, and the state of your mind is a large part of it!
“Andropause” is for those that want to accept it (this is not what I meant when I said your mind plays a big part in it), and lead the lifestyle that promotes it. I know of men in their 60s, 70s and one who is 83 this November in 2016 that are healthier and look more masculine than some men in their 30s (no exaggeration)!
This 83 year old man has more strength in his hand shake than nearly ALL the men, regardless of age, I have shaken hands with (literally hundreds)! So do yourself a favour and look at your diet and lifestyle. This particular 83 year old man has a Mediterranean diet ,rich in olive oil and high in fat- correct, high in fat! Cheese, eggs, fatty meat and fish, lentils, beans and rice, plenty of fresh salads, vegetables and fruit, and which includes alcohol with the main meal! The choice is yours.
Back to the article…
Transdermal Dihydrotestosterone Treatment of ‘Andropause’
Abstract
“Male ageing coincides on average with progressive impairment of testicular function. The most striking plasma changes are an increase in sex hormone binding globulin (SHBG) and a decrease in non SHBG-bound testosterone, which is the only testosterone subtraction effectively bioavailable for target tissues. In healthy subjects the bioavailable testosterone declines by approximately 1% per year between 40 and 70 years but a more pronounced decline has been observed in non-healthy groups, especially in high cardiovascular risks groups. Relative androgen deficiency is likely to have unfavourable consequences on muscle, adipose tissue, bone, haematopoiesls, fibrinolysis, insulin sensitivity, central nervous system, mood and sexual function and might be treated by an appropriate androgen supplementation. The potential risk for prostate has been the main reason for limiting indications of such treatment. Testosterone (T) and dihydrotestosterone (DHT) are two potent androgens which have opposite effects regarding aromatase activity, an enzyme present in prostate stroma and suspected to have a pathogenic influence through local oestradiol synthesis. T is the main substrate for aromatase and oestradiol synthesis while DHT is not aromatizable and, at sufficient concentration, decreases T and oestradiol levels.
A 1.8 years survey of 37 men aged 55-70 years treated with daily percutaneous DHT treatment suggested that high plasma levels of DHT (> 8.5 nmol/l) effectively induced clinical benefits while slightly but significantly reducing prostate size.
Early stages of prostate hypertrophy require synergic stimulation by both DHT and oestradiol, and suppressing oestradiol instead of DHT seems easier and better adapted to the specific situation of aged hypogonadic men. Since the little Information we have related to vascular risks also suggests that aromatase activity and oestradiol induce unfavourable effects, DHT may be considered an attractive alternative for long-term treatment of andropause”
Well there you have it. DHT will reduce prostate size when administered long term (15% reduction).
It seems like we have conflicting reports. On one hand, reducing DHT, is believed to be helping men with enlarged prostates. On the other, giving them a DHT supplement seems to be better with less side effect. What is going on?
Well first off, increasing DHT will increase the ratio of androgens to estrogens. More DHT is not a bad thing as many believe. Second it seems that DHT will reduce testosterone, and thus conversion to estrogen through aromatase action, having the secondary effect of reducing estrogen. It also appears that prostate enlargement requires both estrogen as well as DHT. When the ratio of androgens to estrogens shifts to the estrogen side in men, they appear to have problems.
Reduce DHT (like our drug of interest does) and you see increased high grade cancer. Increase DHT and thus reduce estrogen as a secondary benefit, and you have better results (with no side effects).
Most importantly, you do not have increased “side effects”, such as HIGH GRADE prostate cancer, “breast cancer” in men, male reproductive problems, and all the other side effects we mentioned earlier!
If you think that was a conflicting scenario, here is what the “experts” will tell you about Finasteride.
Prostate Cancer Prevention Trial (PCPT):
Finasteride will:
Lower low grade prostate cancer, but simultaneously increase high grade aggressive cancer. Then they state they don’t know if finasteride causes more aggressive tumours or merely changes the appearance under a microscope to make them look like high grade tumours.
Follow up studies make more assumptions: The reduction in prostate volume makes tumour detection easier, thus we have statements like “the increase in high-grade tumours in the finasteride arm [group] is an artefact [just a perception, but not real]”
That might be the case, but if it is, the mortality rates would indicate this.
78.0% survival rate in the finasteride group versus 78.2% survival in placebo.
Surely if detection is better in the finasteride group than placebo, then the aggressive cancers would progress undetected further in the placebo, and thus kill more in that group than in the drug group. This is simply not the case, instead they report that the mortality rate is about the same! In other words, whether you take this drug or not, your chance of death by prostate cancer is about the same, but the difference is on the drug you have high grade aggressive cancers!
The men in the placebo group died from prostate cancer due to low detection (supposedly), whereas the men in the finasteride group died from high grade prostate cancer, even though they were detected “easier” supposedly.
Why would they go out of their way to spend millions in follow up studies? Maybe because thousands of men all around the world are suing Merck for “side effects” caused by this drug. (Yes, the follow up studies are not done directly by Merck, but that would make things a little too obvious, don’t you think?)
They need to convince people that their drug is safe, in order to keep their profits safe!
Here is a statement by one such law firm in the USA:
“The Product Liability & Defective Drug Litigation Group at our law firm is an experienced team of trial lawyers that focus on the representation of plaintiffs in Finasteride lawsuits. We are handling individual litigation nationwide and currently accepting new sexual dysfunction and cancer cases in all 50 states.”
What has this got to do with male pattern baldness?
Well for starters, the confusion seen in the studies on prostate size and reduction of DHT versus addition of DHT is similar in the hair loss research area. Remember that testosterone is converted to DHT in the local scalp environment by the 5a reductase enzyme family.
There are not many studies showing testosterone effect on balding men. One study did exactly that… in 1968.
The testosterone in this study (and the next) was an ester form called testosterone propionate (propionic acid attached), which requires an enzyme to cleave the ester and release the active testosterone, thus extending the half-life of the testosterone. Once released from the ester, the testosterone can be converted to DHT just like the testosterone produced by the body.
The Ineffectiveness of Testosterone in Male Pattern Baldness
Ronald C. Savin, MD (1968)
(Note: 50% of patients disagree with the title of this article)
ABSTRACT
In a study of male pattern baldness 27 men used 1% testosterone propionate topically for 5 to 21 months with negative results. No patients demonstrated regrowth of hair. Approximately 50% of these patients subjectively noted decrease in rate of hair loss. This latter finding is difficult to evaluate, but is certainly not substantiated by scientific evidence.
If DHT were the only cause of hair loss, would 50% of men receiving topical testosterone to their scalp report “less hair falling out”? The modern theory would predict increased hair loss not a decrease.
Well here is another study that contradicts this, and says testosterone application stimulated hair growth!
(From 1965)
Stimulation of Hair Growth by Topical Application of Androgens
Christopher M. Papa, MD; Albert M. Kligman, MD, PhD
Our previous study of senile skin showed the capacity of topical, but not systemic, testosterone propionate to stimulate hair growth in the axilla and on the forearm. As an extension of this finding, androgen creams were applied to the scalps of 21 bald men. Approximately 75% of the group showed some stimulation of hair growth, as indicated by longer, thicker, more pigmented hairs in the bald area. Within five months of treatment approximately 10% to 15% of the follicles were stimulated to produce terminal type hairs. The probability of regrowth is dependent neither on the duration of the baldness nor on the age of the subject. The enhanced growth is not thought to be an expression of the hormonal activity of testosterone, which in predisposed subjects is a prerequisite for common baldness, but rather a pharmacological local effect on the synthetic activities of the underlying connective tissue. These results indicate the possibility of effective prophylaxis against common baldness; however, indiscriminate use of topical testosterone for its treatment, at this stage, is unjustifiable.
So there you have it.
The scientific literature is full of such seeming contradictions (and their own interpretation of results, even though they admit they do not understand what is going on!). Sometimes the interests with a stake (big business) produce this confusion, by buying people with high positions and titles, such as “professors and doctors”. As a matter of fact, most funding is granted to those who work for the cause of industry, which does not necessarily include the health and wellbeing of people when billions of dollars are involved.
Sometimes people just do not understand what is going on, and thus we get conflicting results.
The most logical explanation for the disease state in men is the ratio of DHT/Testosterone.
Here we see the Free DHT/Free Testosterone ratio, and notice it is high from birth to before puberty and then stabilizes during and after puberty, remaining constant throughout life for men. This graph does not portray absolute amount but rather a ratio. Thus DHT is higher than testosterone at birth.
This consistency is for healthy men, and departure from this physiological balance is believed to cause disease. There are obviously many more hormones that determine health and disease balance.
DHT and testosterone both increase (the absolute amounts increase, the ratio of DHT to Testosterone decreases then plateaus off) till about 25 years of age and then start to decrease, with DHT showing a greater and more dramatic decrease after age 45. It is about this age and after, that men start to have prostate problems. This is when estrogen is seemingly dominating.
Hair loss, on the other hand can occur earlier, starting as early as 20 years of age at about 20% of men, and increasing about 10% per decade thereafter.
Thus at age 50, about 50% of men suffer from androgenetic alopecia. Note that the DHT/testosterone ratio remains the same. That it decreases in some men is due to the bad diet, exercise and sleeping patterns that modern younger and older men alike develop and genetic pre disposition.
In particular weight gain, specifically fat gain, is a problem. The fatter one gets the lower the testosterone, as fat rich in aromatase converts free testosterone to estrogens- but again not all fat people are bald, and many thin men are bald.
Mainstream Medicine still has no clear picture why men lose their hair!
Yes it is related to androgens, but how?
The solution to health is simple, once you understand the cause of the disease.
I do not consider finasteride/Propecia a cure for baldness, as the side effects are 100 times worse than a nice bald head! Also as mentioned, Propecia will become ineffective after about 2 years of use, and hair will start to fall out at an even faster rate after this!
Let me show you a picture and ask some questions:
Is this man bald? Yes
Is it androgenetic alopecia? Yes
Does this man look like he has high testosterone? No
Does he look like he has high androgens? No
High DHT? Probably not
High local DHT production on scalp? Maybe
Is he obese/ overweight? Yes
Are his muscles small? Yes
What is going on here?

I am not saying all males that are bald look like this!
Also today, with the prevalence of steroid use, it is hard to tell who looks like what!
One thing is for sure, the man pictured does not suffer from high blood level of free testosterone, free DHT or any other androgen! Yet he is bald!
It is more probable that he suffers from estrogen dominance. The truth is that the DHT increase = baldness theory resulted from the observation of a genetic condition with low/no levels of the enzyme type II- 5a-reductase.
It is also true that there are other metabolites of this enzyme. The fact that 5a reductase is missing, does not mean it is DHT, even though numerous studies show that DHT addition to cultured hair follicles causes them to “miniaturise” and thus enter what is called catagen phase and finally the telogen phase which is the dormant hair follicle state. The answer to this puzzle will surprise many, and like all solutions, it is elegant!
In case that was not clear, here is a man with normal to high testosterone:
Can you see the difference? Well we can’t see his hair, but that is not the point.
What about this man, before and after?

Low estrogen (left), High estrogen (right)? Same guy different body, same hair. Photoshop? Steroids? The answer might surprise you.
This is Drew Manning. He became famous for wrecking his body on an all junk food, take away fast food, eat what you like, and drink what you like diet.
The picture to the left is actually what he used to look like before the junk diet and lifestyle, and within 6 months of the junk diet and no exercise, he became the fatty you see on the right. Then he spent 6 months transforming himself back to his healthy good looking lean state.
The point is that we are in control of what we look and feel like, and it’s not up to chance alone! It would have been interesting to see if he noticed more hair falling out or if he would develop male pattern baldness on this bad diet and lifestyle, if he were to continue for a few years.
Also, I do not trust people 100%. There might be some “special supplements” this man was taking, that he decided to stop. This coupled with no exercise and a bad diet would equal the result we see too.
There are many guys with bad diets and even exercise routines, but they get good results on steroids. But that is only for a short time. Eventually their bad habits catch up, and they end up worse off.
The point: testosterone and estrogen balance in men.
We are surrounded in a world saturated with estrogenic compounds. For example, when was the last time you received a receipt for something you purchased? Most people receive these receipts every day. They appear harmless enough and simple enough; a mere piece of paper that is activated by heat to show printed information.
This same thermal paper is used for labels, like those used on medication bottles, which includes handling 2 -3 times a day for some people.
The offending chemical is the well known bisphenol A, known as BPA. BPA is found in plastic water bottles, dental composites, resin and plastic used to line metal food and drink containers, lids, caps and thermal paper receipts!
So what exactly is BPA? BPA is an endocrine disruptor. It basically disrupts your hormone balance! It is considered an environmental contaminant, and found in most people’s urine, indicating everyday exposure from many different items.
There is also one called BPS, the one many manufacturers switched BPA for when it got into the news. BPS has similar catastrophic effects on hormone regulation, but now industry can put a BPA FREE label and use BPS instead. See how that works? They now sell more product (they all of a sudden have a competitive market advantage favourable for the average person) containing BPS or some other chemical they replace BPA with.
This might not seem like a big deal, but when you consider that hormones are active on the Nano and pico level (A Nanoliter is one billionth of a litre and a Picoliter is one trillionth of a litre), then it becomes a big deal.
To put that into perspective it would be the same as adding ¼ of a millilitre in an Olympic size pool of 2500000 litres!
This is especially true in the case of BPA, since BPA is intentionally added to the print paper to aid as a print developer at very high doses.
We are talking about 20 mg BPA per gram of paper!
This 20mg is 20 million to 20 billion times over the level that hormones are active in the human body. This would be the same as adding 5000 litres (instead of ¼ ml) to our Olympic swimming pool.
Research also found that when one cleaned/washed their hands with a sanitiser, and then held the receipts, the level of BPA absorbed was much higher and very rapid!
In one experiment, volunteers washed their hands before or after they ordered French fries and picked up the receipt. The level of BPA was found to be 7 nanograms in blood and 20 micrograms per gram of creatine in urine!
The real tragedy of this issue is that people become “sensitised” and “accustomed” to the idea that it is everywhere, so there is nothing they can do, thus forget about it all together and go back to what they would normally do. The same goes for the media, when something is discovered, it is announced (so they can seem just and informative) and then quietly forgotten.
I have seen people put these receipts in their mouth as they put their cash away in their wallets.
What does this mean for hair loss?
For the average Joe, combine this with all the other sources and you have hormone disruption occurring. All these industrial chemicals, BPA , BPS etc.…(there are hundreds) are largely estrogenic. They will bind to and activate estrogen receptors, and produce estrogenic effects. If your work at a cash register, handing out recepts to people all day, you will have significant hormonal problems.
Since hair loss is currently viewed on the level of local hormone disruption on the scalp, this might be a significant contribution to hair loss in some way yet to be discovered.
This is where Imbalance of hormones can destroy your health not just your hair. For example, it was found that BPA can disrupt the rhythm of heart cells just by interacting with estrogen receptors (Figure B below).
Experimental studies have proved that BPA exposure results in the development of arrhythmias in female rodent hearts. Long term exposure to BPA results in cardiac remodelling, atherosclerosis, and altered blood pressure in rodents.
ERB = estrogen receptor B.
The lesson is to be prudent throughout the day, being conscious of the choices you make and how you execute them.
Going back to Drew Manning
As was stated above, he went from fab to fat in 6 months just by altering his diet and lifestyle.
Do you think that his hormone profile changed as well? I would say absolutely 100%. The food we eat has a large effect on our hormone levels and balance.
We do not have his hormone levels before and after, but I would be sure his testosterone levels dropped and estrogen increased in those short few months as he describes having mood swings, irritability and other symptoms related to hormone changes.
Also, fat is rich in aromatase that converts free testosterone to estrogen; I guarantee he had more estrogen and less testosterone in his body.
Maybe Drew would look like this, if he continued his bad diet over years?

These guys are great mechanics, and I love their show, but they are all bald, and overweight, and have bad eating habits and diets.

Would you like to know something ? Those cheese balls will make you fat, but not because they are “high in calories”.
As a matter of fact, calories are not making you fat- sound contradictory?
This will be explained elsewhere.
Estrogen & Hair Loss?
Some of you might be thinking that this all sounds too far fetched to be true. After all, women have higher estrogen than men and they do not have the same rate of baldness as men. When was the last time you saw a bald woman? Exactly.
Reality is not so simple. Obviously women have higher estrogen, but they are not men. It is specifically the male hormone system and its deregulation or disruption from normal that contributes to male pattern baldness.
Before you make up your mind, let me share some research that does prove estrogen and the estrogen receptors are a key factor when it comes to hair growth.
Research by Smart and others in 1996 did provide a link between estrogen and hair growth retardation.
Researchers placed estrogen (estradiol) on the backs of mice after shaving their hair. The mice treated with estrogen arrested the hair follicles in telogen, and had a profound inhibition of hair growth. This temporary baldness was reversed when the mice were treated with an antagonist.
Hair Growth Vs Estrogen
The graph shows the percent of mice with full hair growth. The 17-B-estradiol is the hormone of interest. As you can see, no mice regained hair growth during the 16 weeks (red arrow).
The picture with the mice shows the effect of estrogen on hair growth. Clearly the effect of estrogen can be seen in the top picture.
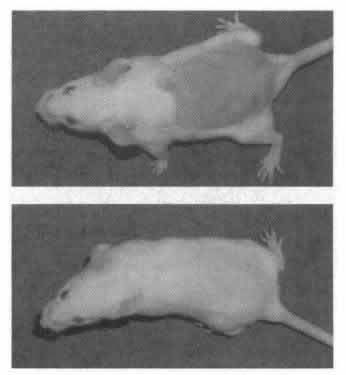
Top: Mouse treated with estrogen. Bottom = normal hair growth.
It is obvious that the sex hormones play an important key role in the regulation of male and female hair loss. What is actually going on in male pattern baldness is a little more complicated than simple (but yet destructive) estrogen dominance, but there is a strong possibility that estrogen dominance is a key player.
What we know about Male Pattern Baldness
Male pattern baldness is dependent on a balance of hormones, often associated with personal lifestyle choices, but not always the case. For example, staying up all night looking at your computer screen will affect melatonin production, causing many hormonal imbalances which can lead to hair loss. On the other hand there are a number of known factors that will cause your hair to fall out! It is not only the local environment on the scalp determines the outcome and fate of hair follicles, but the overall body environment and health of the body.
The method of preference is one in which the local scalp micro environment is brought back to normal by taking advantage of the individuals own hormone system. Preeminent scientists have a clearer picture of how baldness and disease is related. For a consultation please call us.
Whatever the underlying cause of baldness is, it appears that the induced and contained growth factors in one’s blood has the ability to stimulate hair regeneration and stop hair falling out thus stopping the progression of male pattern baldness.
The growth factors stimulate hair regeneration, increased blood flow and vascular growth to hair roots, collagen stimulation wrinkle reduction and normalisation of local scalp immune function and pigmentation. This is coupled with a supplemental and diet program designed to guide your body back to overall health. This is also complimented with a topical solution to nourish, aid and stimulate hair growth.
This 3 phase implementation is what makes Preeminent one of the best places for stopping and reversing baldness.
If you are experiencing hair loss, dont wait another minute. Call now for your free no obligation consultation!
We almost forgot, we offer expert service (Scientist and registered nurses), at the lowest prices you will find in Australia (Probably the world).
The world might not have a magic pill for male pattern baldness, that does not produce side effects worse than the bald head, but the scientists at Preeminent are working on it.
At this time, the Preeminent GFOR treatment is the best medical science has to offer, without resorting to transplant surgery!
At this point – Your Own Blood Holds the Key to Stopping & Reversing Baldness
Whatever the true cause of male pattern baldness, one treatment is fast gaining notorious achievement in being able to stop hair loss and re-grow your own hair!
The procedure involves taking some blood from you and activating and extracting the growth factors.
Once completed, these growth factors are applied to your scalp. The results are remarkable!
These growth factors will not only grow your hair, but will reduce and resolve chronic infections, reduce wrinkles and stimulate collagen formation. This science will also reduce and resolve scarring!
Please take a look at this before and after picture – after only one session of Preeminent regenerative GFOR.
Please note- this is not hair transplant! This is not surgery! Preeminent treatment uses cutting edge science to bring your hair back “from the dead” using the growth factors in your blood!
Below we see a 55 year old man with advanced hair loss. He did not think we could restore his hair growth.
He claimed jokingly that “his scalp was dead”!
We proved him wrong!
His scalp before Preeminent GFOR treatment
55 year old male before Preeminent GFOR treatment
This is his scalp after one Preeminent GFOR regenerative treatment
4 weeks after 1st treatment. Also note that he had a hair cut after the 1st treatment, but the results of our Preeminent science are not due to “over-comb” or longer hair as is used by some of our competitors. Please not the colour of the scalp. The scalp colour (and also hair) is an indicator that melanocytes have been activated. These are the cells that produce melanin in the skin, hair and eyes. These melanin producing cells are a sign of the anagen phase activation in hair, and regeneration of skin on the scalp! – the results were excellent.
Note the pigmentation improvement, wrinkle and plaque elimination,
general scalp health improvement and obviously the increased hair growth, thickness and number.

The scalp of a previously bald 55 year old male after just one Preeminent GFOR treatment (4 weeks after 1st GFOR treatment).
Contrary to what our above client initially thought, the scalp is not “dead” it merely needs to be “guided” back to balance using a combination of scientific synergistic methods.
Please be aware that our clinic has a fully functional laboratory, with a qualified scientist and registered nurse performing the procedure.
Don’t put your results in second best care- talk to preeminent today and see the difference!
Stop waiting, don’t lose another hair!
The time is now, the earlier we treat the scalp the better and faster the result! Do not wait until you are 55!
If you are 20-45 we expect even better results than what you see!
Click here to book an appointment or to discuss your condition over email!
If you prefer to talk, Call us on (02) 8188 4240
If you are losing hair, please remember- Time is Hair! – Preeminent